Robert Frykberg,
DPM, MPH
PRESENT Editor,
Diabetic Limb Salvage
|
|
Preventing Amputations Part 2:
The Comprehensive Diabetic Foot Examination
The Vascular Evaluation
In last month’s issue, we discussed the role of the Comprehensive Diabetic Foot Examination (CDFE) as a means to properly evaluate our patients and thereby assess their risk for diabetic foot ulcer (DFU). While we should all recognize the critically important role of neuropathy underlying the risk for foot ulcers, it goes without question that peripheral arterial disease (PAD) is an increasingly important risk factor for DFU and even more so for amputation. While we will discuss neuropathy at length in a future issue of this eZine, this month, I would like to focus on thevascular evaluation component of the CDFE. My personal belief is that underlying PAD is too often missed in our initial evaluation of diabetic patients – primarily due to the absence of outward signs and symptoms (being masked by coexistent peripheral neuropathy). Many times, the first significant sign of underlying PAD is initially evident upon the presentation of a patient with a new ulceration to our clinics. The PAD is usually not a recent development, but rather, its presence had gone undetected due to the lack of otherwise classical signs and symptoms. Too often, such presentations are at a late stage of critical limb ischemia (CLI). This directly places the limb at risk of amputation should revascularization not be available or indicated for the patient. Hence, the early detection of coexistent PAD becomes a critical component of any amputation prevention program.
The vascular evaluation starts on initial visual inspection of the patient. With the patient seated and legs dependent, look for a very ominous sign of CLI – dependent rubor. (FIGURE 1) Frequently, one extremity will exhibit a normal pink color on dependency, while the ischemic limb will have an erythematous/ruborous appearance on dependency. Of course, one must distinguish such changes from cellulitis (or chronic venous insufficiency when the leg appears cyanotic). Look also for absence of hair growth, shiny skin, and dystrophic appearing nails. In those patients with ulcers, an atrophic appearance to the wound without signs of granulation or bleeding will be the first clinical clue. Raise the leg foot and leg from dependency to a level above the heart. If the sole of the foot blanches white (plantar pallor) on elevation, another important diagnostic clue has revealed itself. Then have the patient sit with legs dependent and determine the time it takes for the veins on the dorsum of the foot to fill (venous filling time). Anything greater than 25 seconds is abnormal, as is a capillary refill time (response to digital pressure against the toe tips) of greater than 3 seconds.
| Figure 1. Dependent rubor. Note the reddish appearance of the left leg and foot on dependency compared to the normal color of the patient’s right foot and leg. |
|
|
Of course, pulse palpation of both the Dorsalis pedis and the Posterior tibial arteries at the foot/ankle level are critical aspects of the vascular examination. At the same time, don’t forget to palpate the Popliteal arteries as well behind the knees. The absence of pedal pulses is a significant indicator of impaired perfusion to the foot. Remember that the classic level for arterial occlusive disease in the diabetic patient is at the level of the tibial arteries below the knee (often called trifurcation disease or infrageniculate disease). Hence, an examiner might find a nicely bounding popliteal pulse in association with absent pedal pulses. This is a classic presentation for the diabetic patient with PAD. Pulse palpation is a skill that varies among examiners, especially when edema is present. Also remember that medial arterial calcification, so common in patients with established peripheral neuropathy, can obscure the pulsatility of peripheral arteries. Nonetheless, most of us can even palpate a pulse on a table if we try hard enough (actually feeling our own pulses). Therefore, when clinical signs indicate ischemia and pulses are even questionable, it becomes necessary to obtain further quantitative confirmation of the circulatory status.
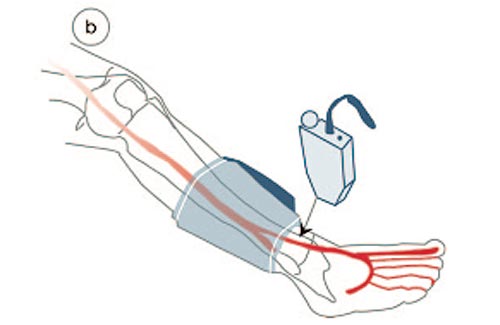
| Figure 2. Acquisition of The Ankle-Brachial index (ABI) of the Dorsalis pedis artery. An ankle cuff is inflated until the Doppler signal is eliminated. Slowly deflate the cuff noting at which pressure the Doppler signal returns. Divide this ankle pressure by the brachial artery pressure obtained in the same way. This ratio is taken as the ABI. The same should be done for the Posterior tibial artery pressure. The highest of the two ratios is considered the clinical ankle-brachial ratio. |
|
|
Measurement of the ankle-brachial index (ABI) is the standard diagnostic quantitative vascular evaluation for the feet. While usually performed at multiple levels on both legs when a formal vascular laboratory study Is requested, the ABI can easily be done in the office or clinical setting as part of your clinical vascular evaluation – especially when you suspect some level of PAD in your patient. This is performed with a standard blood pressure cuff and a hand held Doppler probe (I always keep one in my pocket). Place the cuff just above the ankle joint and inflate until the Doppler signal is eliminated. Slowly deflate the cuff, noting at which pressure the Doppler signal returns. Divide this ankle pressure by the brachial artery pressure obtained in the same way. This ratio is taken as the ABI. The same should be done for the Posterior tibial artery pressure. The highest of the two ratios is considered the clinical ankle-brachial ratio. While an index of 1.1 is considered normal, any ratio below 0.9 is considered indicative of impaired perfusion to the ankle. An ABI less than 0.6 and certainly below 0.5 is considered to be critical ischemia and requires referral for further testing and vascular consultation. Nonetheless, nothing is a certainty in the diabetic patient. While a reduced ABI is always abnormal, a normal one cannot always be considered normal. Due to arterial calcification, ABI measurements are often falsely elevated (greater than 1.2 and often greater than 2.0) in diabetic patients, because of incompressible arteries. This is the reason why toe pressures are often favored as being more reliable than ankle pressure measurements in diabetic patients. It is only arteries larger than those in the toes that succumb to calcification in patients with diabetes. Nonetheless, you need to be aware that ostensibly normalABI measurements can be falsely elevated to normal levels due to associated arterial calcification in association with underlying PAD! So, always be suspicious – when you suspect PAD, look for PAD. If diagnosed or indeterminate, obtain a formal vascular lab study with additional testing as well as a vascular surgical consultation.
PAD can be limb threatening when undetected and untreated- especially in the presence of a DFU. It is our job to detect it through appropriate screenings and evaluation of all ulcerated and infected feet. As the saying goes, “if you look for it, you will find it”.
References are provided below that can expand upon many of the points made above. We welcome your opinions, concerns, and suggestions. If you have an interesting case or a troubling circumstance that you would like to share with fellow PRESENT Diabetes members, please feel free to comment on eTalk.
Best regards,

Robert Frykberg, DPM, MPH
PRESENT Editor,
Diabetic Limb Salvage
REFERENCES

- Pecoraro RE, Reiber GE, Burgess EM: Pathways to diabetic limb amputation: basis for prevention. Diabetes Care 1990; 13: 513-521.
- Reiber GE, Vileikyte L, Boyko EJ, et al.: Causal pathways for incident lower-extremity ulcers in patients with diabetes from two settings. Diabetes Care 1999; 22(1): 157-62.
- Frykberg RG, Zgonis T, Armstrong DG, et al.: Diabetic Foot Disorders: A Clinical Practice Guideline (2006 Revision). J Foot Ankle Surg
2006; 45(Suppl): S2-S66.
- American Diabetes Association: Consensus Development Conference on Diabetic Foot Wound Care. Diabetes Care 1999; 22(8): 1354.
- Boulton AJ, Armstrong DG, Albert SF, et al.: Comprehensive foot examination and risk assessment: a report of the task force of the foot care interest group of the American Diabetes Association, with endorsement by the American Association of Clinical Endocrinologists. Diabetes Care 2008; 31(8): 1679-85.
- International working group on the diabetic foot: International Consensus on the Diabetic Foot. In: Apelqvist J, Bakker K, Van Houtum WH, et al., eds., vol 2005. Maastricht: International Working Group on the Diabetic Foot, 1999.
- Apelqvist J, Bakker K, van Houtum WH, Nabuurs-Franssen MH, Schaper NC: International consensus and practical guidelines on the management and the prevention of the diabetic foot: International Working Group on the Diabetic Foot. . Diabete Metab Res Rev 2000; 16 ((Suppl. 22. 1)): S84 -S92.
|
|