Preventing Amputations Part 3:
The Comprehensive Diabetic Foot Examination
Neuropathy
In the last several issues (Part 1, Part 2 ), we’ve been discussing amputation prevention and the importance of the comprehensive diabetic foot screening examination (CDFE) as an effective method to diagnose persons “at risk” prior to the onset of limb threatening problems. Last month, we focused on the vascular evaluation as a means to detect peripheral arterial disease (PAD), since this complication can be limb threatening in the presence of ulceration, infection, or gangrene. Nonetheless, no discussion about amputation prevention, the diabetic foot, or complications of diabetes would be complete without a concurrent discussion of peripheral neuropathy. Concurrent is probably the correct word to use in this regard, since neuropathy is concurrent with many other complications of the diabetic lower extremity and, in fact, likely precedes them. Diabetic peripheral neuropathy (DPN) is probably the most common complication of long standing diabetes – at least in the lower extremities- and can be present in 45-50% of diabetic patients having the disease for twenty years or more. It is certainly a consequence of long term hyperglycemia, but it can also be attributed to microvascular disease, protein glycosylation, and various nutritional disturbances rendering the diabetic nerve fibers at risk for structural alteration and physiologic dysfunction. Most importantly, DPN is a major, if not the major predisposing risk factor for diabetic foot ulceration (DFU), infections, amputations (in association with PAD and infection), and certainly the diabetic Charcot foot.
Neuropathy is a many splendored thing, meaning that it can affect all the nerves of the lower extremity (as well as elsewhere) and has different presenting signs and symptoms. While DPN can be classified in several different ways, it makes sense to simplify thing as much as possible. The classical sensory neuropathy (somatosensory) of “glove and stocking” distribution leading to loss of protective sensation (LOPS) is the most commonly recognized form of DPN and is, indeed, the most common component cause leading to DFU. However, somatosensory neuropathy can also involve motor fibers leading to atrophy – and recognized by muscle weakness, atrophy, or paresis. While LOPS might be considered a “negative” symptom since there is usually absence of sensation, affected patients can also have “positive” symptoms such as burning, lancinating pains, or cramping. These disturbing symptoms come under the general category of painful neuropathy and the diagnosis is one of exclusion of other causes (such as PAD). However, painful neuropathy, unless accompanied also by LOPS, will rarely cause ulceration.
Autonomic neuropathy (AN) is also an important component of DPN, affecting both sympathetic and parasympathetic fibers. While developing concurrently with large and small fiber somatosensory neuropathy, it is not usually recognized until significant dysfunction has occurred. Important consequences of AN include neurovascular disturbances from “sympathetic failure” where arteriovenous shunts are dysfunctional and allow for impaired (excessive) microvascular blood flow and abnormal thermoregulatory responses. The classic warm, dry neuropathic foot represents this condition well. Anhidrosis- sweat gland dysfunction- due to AN is clinically evidenced by very dry, often callused, and cracked skin on the soles of the feet.
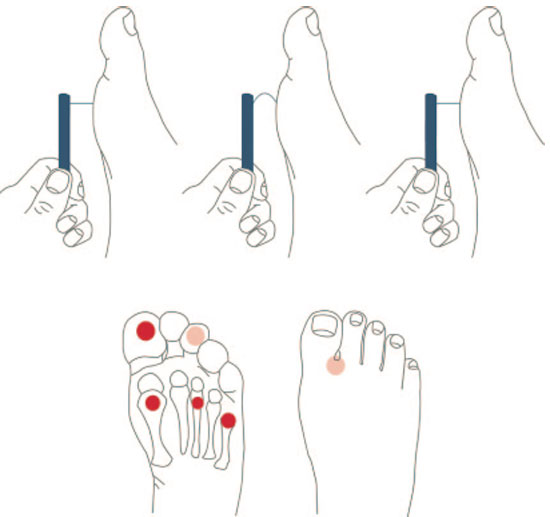
As recommended by the CDFE Taskforce in 2008 (reference 5 below), 5 simple clinical tests can be used to diagnose LOPS. These are listed in Table 1. Most commonly, the simple 10 gram monofilament is used as the primary diagnostic modality, although there are reported problems with reproducibility. Nonetheless, this and one of the other tests/modalities should be used to confirm or rule out the presence of sensory neuropathy. Simply described, the monofilament should be applied to four sites on the plantar surface of the foot until visible buckling of the monofilament is observed. (Figure 1)
Figure 1. Upper panel: For performance of the 10-g monofilament test, the device is placed perpendicular to the skin, with pressure applied until the monofilament buckles. It should be held in place for ~1 s and then released. Lower panel: The monofilament test should be performed at the highlighted sites while the patient’s eyes are closed.
(From: Boulton AJ, Armstrong DG, Albert SF, et al.: Comprehensive foot examination and risk assessment: a report of the task force of the foot care interest group of the American Diabetes Association, with endorsement by the American Association of Clinical Endocrinologists. Diabetes Care 2008; 31(8): 1679-85.) |
|
|
Table 1.: Clinical tests for loss of protective sensation (LOPS)
Neurological assessment 10-g monofilament 1 of the following 4
- vibration using 128-Hz tuning fork
- pinprick sensation
- ankle reflexes
- VPT (Vibration Perception Threshold) using the biothesiometer or neurothesiometer
|
At this point, with the patient’s eyes closed, a “yes” or “no” response to the perception of the filament is requested. Loss of the ability to detect this light pressure at one or more sites has been associated with loss of large fiber function (LOPS). Of course, callused areas should be avoided. The 128-Hz tuning fork is also a very useful and readily available instrument to assess vibratory sensation on the tip of the great (or lesser) toes bilaterally. When a patient cannot detect the vibration that the examiner can clearly feel, neuropathy is diagnosed. Similarly, light pin-prick sensation with a sterile, disposable needle and elicitation of ankle deep tendon reflexes should be performed by standard techniques. Failure to perceive the slight deformity of a pinprick or total absence of ankle reflex either at rest or upon reinforcement is regarded as an abnormal result. Vibration perception threshold (VPT) is determined by applying a biothesiometer to the tip of the great toe with the patient’s eyes closed. (Figure 2) The dial (amplitude) is gradually increased until the patient can sense the vibration. The arbitrary units on the dial indicate the volts at which the perception occurs. A VPT>25 is associated with neuropathy and risk for DFU.
| Figure 2.: Biothesiometer test. |
|
|
The simplest test to detect Autonomic neuropathy/ anhidrosis is with a Neuropadâ. This cobalt blue bandage is applied to an intact area on the sole of the foot for 10 minutes. Normally sweating skin will turn the blue indicator to pink within this time frame. (Figure 3) A very lightly mottled or retained blue color of the indicator pad indicates a lack of sweating consistent with AN.
| Figure 3.: Neuropad® test for anhidrosis (Autonomic neuropathy). |
|
| a) The normal response is illustrated showing the conversion of the indicator pad from cobalt blue to pink in less than 5 minutes. |
b) The normal response is illustrated showing the conversion of the indicator pad from cobalt blue to pink in less than 5 minutes. |
|
|
|
Neuropathy is an extremely important pathology to detect in your screening examination and probably the easiest to detect clinically by using the methods described. Make this a standard part of your examination protocols for your diabetic patients and you will be doing your patients a great service – and practicing the art of Amputation Prevention.
References are provided below that can expand upon many of the points made above. We welcome your opinions, concerns, and suggestions. If you have an interesting case or a troubling circumstance that you would like to share with fellow PRESENT Diabetes members, please feel free to comment on eTalk.
Best regards,

Robert Frykberg, DPM, MPH
PRESENT Editor,
Diabetic Limb Salvage
REFERENCES

- Pecoraro RE, Reiber GE, Burgess EM: Pathways to diabetic limb amputation: basis for prevention. Diabetes Care 1990; 13: 513-521.
- Reiber GE, Vileikyte L, Boyko EJ, et al.: Causal pathways for incident lower-extremity ulcers in patients with diabetes from two settings. Diabetes Care 1999; 22(1): 157-62.
- Frykberg RG, Zgonis T, Armstrong DG, et al.: Diabetic Foot Disorders: A Clinical Practice Guideline (2006 Revision). J Foot Ankle Surg
2006; 45(Suppl): S2-S66.
- American Diabetes Association: Consensus Development Conference on Diabetic Foot Wound Care. Diabetes Care 1999; 22(8): 1354.
- Boulton AJ, Armstrong DG, Albert SF, et al.: Comprehensive foot examination and risk assessment: a report of the task force of the foot care interest group of the American Diabetes Association, with endorsement by the American Association of Clinical Endocrinologists. Diabetes Care 2008; 31(8): 1679-85.
- International working group on the diabetic foot: International Consensus on the Diabetic Foot. In: Apelqvist J, Bakker K, Van Houtum WH, et al., eds., vol 2005. Maastricht: International Working Group on the Diabetic Foot, 1999.
- Apelqvist J, Bakker K, van Houtum WH, Nabuurs-Franssen MH, Schaper NC: International consensus and practical guidelines on the management and the prevention of the diabetic foot: International Working Group on the Diabetic Foot. . Diabete Metab Res Rev 2000; 16 ((Suppl. 22. 1)): S84 -S92.
|
|